A woman shows up at the emergency department feeling breathless and sweaty. She feels a pain in her back, near her shoulder blade, that radiates down her left arm.
All her tests come back normal, though, and she is sent home.
The next day, she sees a cardiologist. He notes that her symptoms might be anxiety-related.
That night, she suffers a heart attack.
This is Barbara Collura's story – an ambassador at the Family Heart Foundation in the United States – but it is also the fate of thousands of other women around the world.
While Collura eventually received the care she needed, the gender gap in cardiology care is costing other women their lives.

In some wealthy nations with robust medical systems like Australia, researchers estimate up to 20 percent of heart attack deaths in women could be avoided if the gender gap were closed and all patients were treated the same.
But they are not. Women under 55 in the US are seven times more likely than men to be sent home from the emergency department without proper cardiac testing.
During diagnosis, a single word may be putting them at risk: Atypical.
For decades now, doctors have deemed women's heart attack symptoms as 'atypical' because they can differ from the symptoms of men.
In reality, however, there is nothing atypical about symptoms that impact half the population. Besides, the core symptom is the same, regardless of gender.

Recent observational studies and prospective trials have shown that more than 90 percent of women and men report chest pain during a heart attack.
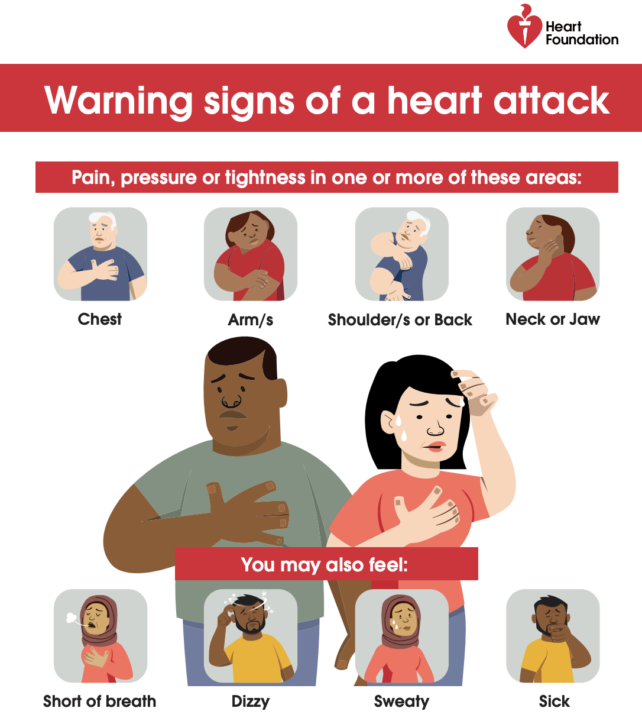
The difference is that women are also more likely to experience nausea, breathlessness, fatigue, jaw pain, or pain between the shoulder blades at the same time – and these symptoms can muddy the diagnosis.
If a symptom pattern is deemed 'atypical', a physician may misinterpret the signs as 'unusual' or as probably unrelated to the heart.
But using the male body as the norm for diagnosis and care can prove deadly.
Renowned cardiologist Stephen Nicholls, who leads Australia's Victorian Heart Hospital, is one of many doctors worldwide who think the term 'atypical' is outdated and needs to be changed.
"Despite widespread promotions of the importance of heart disease in women, there remains a view in the community that heart disease is a problem for men alone," Nicholls told ScienceAlert.
Cardiovascular disease, however, is the number one killer of females in the US today, and it leads to a similar number of deaths in women as in men.
Nevertheless, studies show that compared to men, women with heart attack symptoms are less likely to be prescribed aspirin, be resuscitated, or receive ambulance transport to the hospital using lights and sirens.

The disparity even has a name: Yentl syndrome. The term was first coined in 1991 by the American cardiologist Bernadine Healy, who took the title from a film featuring Barbara Streisand.
The main character disguises herself as a man to attend school and receive the same education as her male peers.
More than three decades later, the field of cardiology is still struggling to move beyond Yentl syndrome and the male-default model of heart attacks.
Many of today's heart attack guidelines, such as those around aspirin, are based on past studies that predominantly enrolled men.
Oftentimes, risk factors that specifically impact women, like menopause, polyendocrine metabolic ovary syndrome (previously known as PCOS), and pregnancy-related conditions, are not included in clinical assessments of heart attack risk.

"We have much more work to do to reduce the burden and outcomes of heart disease for women in the community," Nicholls told ScienceAlert.
While it is true that outward signs of heart attacks in women can differ to men, there is a key similarity: chest pain.
In popular culture, chest pain from a heart attack is often illustrated as crushing and debilitating.
But cardiologist Michelle O'Donaghue at Brigham and Women's Hospital in Boston and Harvard Medical School says it is a common misconception that all heart attacks are dramatic.
Because of this misunderstanding, patients may dismiss their own symptoms or not take them seriously enough if they don't present in a certain, stereotypical way.
"In reality, [heart attacks are] often quieter and more gradual, which is exactly why they're missed," O'Donaghue told ScienceAlert.
In fact, O'Donaghue says women often describe the chest pain as dull or heavy 'pressure' that lasts for a few minutes and then fades away. Similar to Barbara Collura's story, women are more likely to suffer heart attacks during rest or sleep.
"We know that women are more likely to experience less common symptoms like nausea, shortness of breath, and jaw or arm pain- symptoms that don't immediately signal 'heart attack' to patients or clinicians," Donaghue added.
"Women may be more likely than men to describe more subtle or diffuse symptoms, which can be intermittent and easier to overlook."
When experiencing a heart attack, studies show that women tend to experience higher odds of pain between the shoulder blades, nausea or vomiting, and shortness of breath. These 'atypical' symptoms may explain why they are more likely to be misdiagnosed or sent home without care.
As a 2020 study notes, physicians begin the diagnostic process by intuitively recognizing familiar symptoms of heart attacks.
When these symptoms combine to create 'unique' patterns, however, it can often lead to misdiagnosis.
"While the majority of people, both men and women, experience chest pain when they have heart disease, women are more likely to experience additional or alternative symptoms such as breathlessness, nausea, fatigue, anxiety, and palpitations," Nicholls explained.
"It certainly can make diagnosis more challenging, but there is increasing emphasis in guidelines and education about the potential relevance of these symptoms."
While newer guidelines do acknowledge these other symptoms of cardiac arrest and are moving away from the term 'atypical', change has been slow. The message still needs to be spread.

Related: Huge Study Links 99% of Heart Attacks And Strokes With 4 Risk Factors
Barbara Collura only received a diagnosis on her third visit to the doctors, after she had already had a heart attack. Her artery was 99 percent blocked.
As a Heart Foundation ambassador, Collura is now sharing her story in the hopes of saving other women's lives.
If someone is worried they are having a heart attack, O'Donaghue says that patients should trust their instincts.
"In particular, seek urgent care for any new, unexplained symptoms, including chest discomfort or shortness of breath that persists or comes and goes," she told ScienceAlert.
"It's always better to err on the side of caution. If you think you may be experiencing a heart attack, never drive yourself to the hospital – it's always best to call 911."